PCOS: Symptoms, Causes, and Risk Factors Every Woman Should Know
PCOS: Symptoms, Causes, and Risk Factors Every Woman Should Know
A young woman in Lagos notices her period hasn't come in three months. She's not pregnant. She's been gaining weight around her belly despite eating the same way she always has. Her chin keeps breaking out like she's a teenager again, and lately she's been finding more hair on her pillow than she's comfortable with.
She visits a clinic. The doctor mentions something called PCOS.
She's never heard of it.
She's not alone. Polycystic ovary syndrome affects between 8 and 13% of women of reproductive age worldwide, and according to the World Health Organization, up to 70% of cases go completely undiagnosed. In Nigeria and across much of Africa, that number is likely even higher, partly because period irregularities are often dismissed as stress, spiritual issues, or "just how some women are."
PCOS is none of those things. It's a real, diagnosable hormonal condition, and understanding it could change the trajectory of a woman's health for the rest of her life.
What Is PCOS?

Polycystic ovary syndrome is a hormonal and metabolic disorder that disrupts the normal rhythm of a woman's reproductive system. The name is a bit misleading. Despite what it sounds like, you don't need to have cysts on your ovaries to have PCOS. What's actually happening is more complex than that.
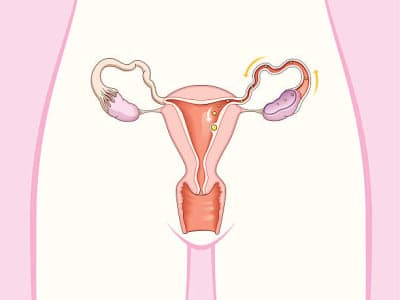
In a normal menstrual cycle, the ovaries release an egg roughly once a month. In women with PCOS, that process breaks down. The ovaries produce too many male hormones called androgens, which interfere with ovulation. Instead of releasing a mature egg, the ovaries end up holding onto several small, undeveloped follicles. On an ultrasound, these look like tiny pearls arranged around the edge of the ovary. Not dangerous, not painful, but a visible sign that ovulation isn't happening the way it should.
PCOS doesn't affect every woman the same way. Some women have all the classic signs. Others have just one or two. That variability is part of why it takes so long for many women to get a proper diagnosis.
Early Signs and Symptoms of PCOS
Menstrual Symptoms of PCOS
The most telling sign of PCOS is an irregular menstrual cycle. We're talking fewer than 9 periods in a year, cycles that stretch beyond 35 days, or periods that arrive unpredictably with no pattern whatsoever. For some women, periods stop altogether for months at a time.
In Nigeria, it's common for women to attribute skipped periods to stress, travel, or even "the heat." And while those things can cause occasional cycle shifts, persistent irregularity is a different story and deserves proper investigation.
Physical Symptoms of PCOS
Excess facial or body hair (hirsutism): This affects up to 70% of women with PCOS. Hair grows in places it typically doesn't in women, including the chin, upper lip, chest, and stomach. It's caused by elevated androgens and is one of the most emotionally distressing symptoms women report.

Acne: Not teenage breakouts that clear up in a few weeks. PCOS acne tends to be persistent, deep, and concentrated along the jawline and chin.

Hair thinning on the scalp: The same androgens that cause excess body hair can thin the hair on your head, following a pattern similar to male-pattern baldness.

Weight gain around the abdomen: Not generalized weight gain but specifically around the belly, even in women who aren't eating excessively.

Dark velvety skin patches: Known medically as acanthosis nigricans, these patches appear around the neck, armpits, or inner thighs and are a visible sign of insulin resistance.

Hormonal and Metabolic Symptoms of PCOS
This is the part that most women don't connect to their periods at all. PCOS is not just a reproductive problem. It's a metabolic one too. Insulin resistance affects between 65 and 95% of women with PCOS, even those who are not overweight. When the body stops responding properly to insulin, blood sugar rises, the pancreas works overtime, and the ovaries get flooded with signals to produce even more androgens. It's a cycle that feeds itself.
Emotional and Mental Health Symptoms of PCOS
Anxiety, depression, and body image struggles are significantly more common in women with PCOS than in the general population. This isn't just about coping with physical symptoms. The hormonal imbalances themselves affect mood regulation in real, measurable ways. Yet this part of PCOS rarely gets discussed in clinical settings, especially in environments where mental health already carries stigma.
What Causes PCOS?
There is no single cause. PCOS is what doctors call a multifactorial condition, meaning several biological processes interact to create it. No one factor explains every case.
The Role of Insulin Resistance in PCOS
Insulin is the hormone that helps your body use sugar from food as energy. When cells stop responding to it properly, the body produces more and more insulin trying to compensate. That excess insulin acts like a signal flare to the ovaries, telling them to ramp up androgen production. More androgens mean more disruption to ovulation, which is how insulin resistance, a condition most people associate with diabetes, ends up sitting right at the center of a reproductive disorder.
How Excess Androgens Drive PCOS Symptoms
Androgens are often called "male hormones," but every woman's body produces them in small amounts. In PCOS, the ovaries and sometimes the adrenal glands produce far more than they should. That excess is what drives the acne, the unwanted hair growth, the hair loss, and the ovulation problems. It's not one symptom causing another. It's one root hormonal disruption expressing itself in many different ways across the body.
Is PCOS Genetic?
Strongly, yes. Twin studies suggest PCOS has up to 70% heritability. If your mother, sister, or aunt has PCOS or type 2 diabetes, your own risk is meaningfully higher. Specific gene variants affect how the body regulates hormones, processes insulin, and develops follicles in the ovaries. This doesn't mean PCOS is inevitable if it runs in your family, but it does mean awareness and early monitoring matter more.
Environmental and Lifestyle Triggers
Genetics loads the gun, but lifestyle and environment often pull the trigger. Poor dietary patterns, physical inactivity, disrupted gut health, exposure to certain environmental pollutants, and chronic stress can all push a woman who is genetically susceptible toward developing PCOS. In urban Nigerian settings where ultra-processed foods have become staples, where heat and congestion make outdoor exercise difficult, and where chronic stress is almost a default state, these environmental pressures are worth taking seriously.
PCOS Risk Factors: Who Is Most Likely to Develop It?
Family History and PCOS Risk
Having a first-degree relative with PCOS or type 2 diabetes increases your risk considerably. PCOS tends to cluster in families, and the metabolic component follows the same pattern.
Weight, Lifestyle, and PCOS Risk
Between 38 and 88% of women with PCOS are overweight or obese. Excess weight worsens insulin resistance, which amplifies every hormonal disruption downstream. That said, lean women develop PCOS too. Weight is a risk factor and a complicating factor, not a prerequisite.
PCOS Risk in Teenagers and Young Women
PCOS can begin showing signs as early as the very first menstrual period. In adolescents, irregular cycles and acne are often written off as normal puberty adjustments. Sometimes they are. But when those symptoms persist beyond two years after the first period, or when excess hair growth or significant weight gain enters the picture, PCOS should be on the table as a possibility.
How Is PCOS Diagnosed?
There is no single test for PCOS. Diagnosis is based on what clinicians call the Rotterdam criteria, which requires at least two of the following three features after other conditions have been ruled out:
Clinical or biochemical signs of elevated androgens (hirsutism, acne, or a blood test showing high androgen levels)
Ovulatory dysfunction (irregular or absent periods)
Polycystic ovarian appearance on ultrasound or elevated AMH levels on a blood test
Additional tests typically include hormone panels, blood glucose and insulin levels, lipid profiles, and blood pressure checks. In adolescents, ultrasound is not recommended for diagnosis because polycystic-looking ovaries are common during puberty and don't carry the same significance.
Access to these tests varies widely across Nigeria. Many women in smaller cities or rural areas may not have access to hormonal blood tests or quality ultrasound. This is a real barrier, and it's one reason so many cases go undiagnosed for years.
Long-Term Health Risks of Untreated PCOS
This is where PCOS stops being just a period problem and becomes a whole-body concern.
Women with PCOS face significantly elevated risks for type 2 diabetes, with over 50% developing it by age 40. Cardiovascular disease risk is higher, including hypertension and abnormal cholesterol levels. Because irregular periods mean the uterine lining isn't being shed regularly, the risk of endometrial hyperplasia and endometrial cancer rises over time due to prolonged exposure to estrogen without the balance of progesterone.
Mental health complications, including anxiety, depression, and disordered eating are also considerably more prevalent in women with PCOS, though they remain among the least addressed aspects of the condition in clinical practice.
When to See a Doctor for PCOS Symptoms
If you've been experiencing irregular periods for more than a few months, noticing unusual hair growth or stubborn acne, struggling with unexplained weight changes, or having difficulty conceiving, those are reasons to get evaluated now, not later.
Early diagnosis and management reduce virtually every long-term risk associated with PCOS. Lifestyle changes alone, particularly around diet and regular movement, can significantly improve insulin sensitivity, regulate cycles, and reduce symptom severity even before any medication is introduced.
You don't need to wait until things get severe. You just need to start the conversation with a doctor who takes your symptoms seriously.

PCOS Symptoms Checklist
Periods fewer than 9 times per year or cycles longer than 35 days
Periods that stopped for 3 or more months without pregnancy
Excess hair on the face, chest, stomach, or back
Persistent acne along the jawline or chin
Thinning hair on the scalp
Unexplained weight gain around the abdomen
Dark velvety skin patches on the neck, armpits, or groin
Difficulty getting pregnant after trying for 12 months or more
Mood changes, anxiety, or persistent low mood tied to your cycle
If three or more of these sound familiar, speak with a gynecologist or endocrinologist.
CONCLUSION
PCOS is not a life sentence. It is a manageable condition that millions of women live with well, once they know what they're dealing with.
The real problem isn't PCOS itself. It's the years many women spend being told their symptoms are stress, spiritual warfare, or simply "how their body is." It's the clinics that don't ask the right questions. It's the silence around women's health that allows a condition affecting 1 in 10 women to stay invisible for decades in a woman's life.
Knowing the symptoms of PCOS, understanding what drives them, and recognizing your own risk factors is not a small thing. It's the difference between a decade of confusion and a clear path toward managing your health on your own terms.
Track your cycle. Notice your body. And if something feels consistently off, trust that instinct enough to get it checked.